
Complex treatment to help a patient with several liver metastasis. In this case a biopsy followed by a microwave ablation of a residual metastasis in segment 1 was performed. Both required extreme precision to not harm critical structures like the inferior caval vein, the right branch of the portal vein and the main bile duct. Successfull treatment was shown on control scans right after the ablation and confirmed by a MRI 6 weeks after the intervention.
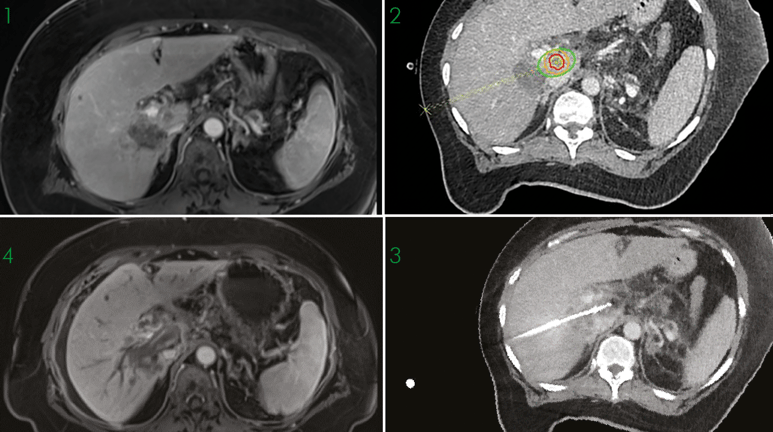
1. Initial MRI scan showing suspected vital tumour in segment I
2. Planing of the trajectory for biopsy and ablation also showing the tumour (red), the safety margin (yellow) and the expected ablation zone (green)
3. Needle validation scan with antenna placed in the tumour
4. MRI scan confirming complete ablation 6 weeks after treatment
2. Planing of the trajectory for biopsy and ablation also showing the tumour (red), the safety margin (yellow) and the expected ablation zone (green)
3. Needle validation scan with antenna placed in the tumour
4. MRI scan confirming complete ablation 6 weeks after treatment
Name: Dr. Lukas Lürken
Institution: University Hospital Regensburg, Germany
Patient age and sex: 56 years, female
Initial condition:
- Aug 2008 first diagnosis: Breastcancer left, treated with selective resection, radiotherapy and hormone therapy
- Nov 2017 diffuse spinal metastasis diagnosed, treated with radiotherapy. Systemic therapy with several changes due to adverse effects
- Oct 2019 Resection of local recurrent tumor left mamma
- Jan 2020 Liver metastasis in segment VI/I
- Apr 2020 Electrochemotherapy (ECT) of the liver metastasis
- June 2020 residual, progressive tumour tissue in Liver segment I in MRI 6 weeks after ECT
- Biopsy of the ablation defect in segment VI as well as biopsy of the suspected vital tumour in segment I, followed by microwave-ablation of the tumour
- Stereotactic navigation with Cas-One IR due to the complicated local tumour situation in Segment I with long trajectory and several “no-go” structures close to the target lesion, such as the inferior caval vein, the right branch of the portal vein and the main bile duct
- First, a 13 G 10 cm coaxial needle was introduced into the liver tissue next to the ECT-Necrosis in segment 6. After biopsy of the necrotic defect with a 14 G SABD biopsy device, the coaxial needle was advanced in the same direction until next to the tumour lesion in segment I, where another biopsy was performed. The biopsy device was removed and a 20 cm microwave antenna was inserted through the coaxial needle. The coaxial needle was retracted for about 5 cm and microwave ablation was performed for 5 minutes with 65 Watts. Control scans directly after the ablation showed complete ablation of the residual tumour. Malignancy of the suspected residual tumour in segment I was confirmed by pathology. The biopsy of the necrotic area in Segment VI showed no vital tumor tissue
Result:
- Complete ablation was achieved, a follow up MRI after 6 weeks confirmed complete ablation
- Unfortunately, the patient’s outlook is not good, since she has a multisystemic metastatic disease, which showed recurrency under several systemic therapeutic regimes. Follow up MRI after 6 weeks showed several new liver metastases and a probably new supraphrenic lymph node metastasis. The patient also developed cholestasis due to the new liver tumors, requiring percutaneous transhepatic cholangiodrainage therapy
- A new regime of combined systemic therapy was discussed
